A). Wetting agents
For the disperse phase to freely and distribute in the continuous phase, it needs to be wetted by the liquid. The presence of entrapped air pockets on the particle surface or if the particles are hydrophobic is a hindrance to dispersion.
Wettability can be enhanced through the reduction of the interfacial tensions, namely solid-liquid and liquid-vapour interfaces.
1. Surface active agents
Surface active agents (surfactants for short) are excipients that lower the surface tension (or interfacial tension) between two liquids or between a liquid and a solid.
Surfactants with HLB values between 7 and 9 have been shown to be suitable wetting agents in pharmaceutical disperse systems.
This is because the apolar groups of the surfactant are able to adsorb onto hydrophobic parts of formulation particle while the polar groups project into the aqueous medium, resulting in a lowering of the interfacial tension between the solid and the liquid.
2. Hydrophilic colloids
Hydrophilic colloids are high molecular polysaccharide polymers or clays. They include acacia, bentonite, tragacanth, alginates and cellulose derivatives.
Being hydrophilic, they are able to coat particles to impart hydrophilic character to the disperse phase. In addition, hydrophilic colloids may also increase viscosity of the continuous phase, reducing the rate of sedimentation of particles.
3. Solvents
Common polar pharmaceutical solvents such as glycerol, propylene glycol and polyethylene glycol and alcohol are highly water-miscible and are able to reduce the liquid-air interfacial tension.
They enable water to infiltrate deep into power agglomerates, displacing entrapped air and enabling wetting of the dispersion to take place.
B). Flocculants
A well-formulated disperse system is one that exhibits the correct degree of flocculation. Systems that are underflocculated generally tend to settle and sediment very rapidly although the compacts formed are loose and redispersion is possible.
On the other hand, overflocculation results in products that while settle slowly the sediments pack tightly such that redispersion is not possible.
By controlling the degree of flocculation, it’s possible to reach a happy medium – in which there is a degree of flocculation and also deflocculation.
This can be achieved through, not only through particle size control and viscosity-modification, but also by using flocculating agents, including electrolytes, ionic surfactants and polymer flocculating agents.
1. Electrolytes
The addition of inorganic electrolytes to the solution changes the zeta potential of the dispersed particles, and provided this is lowered sufficiently enough, will produce a flocculated system.
2. Surfactants
Ionic surfactants can also be used to create flocculation in a disperse system by neutralising particle charges and creating a deflocculated system.
3. Polymeric flocculants
Several polymeric excipients are capable of forming gel-like networks in disperse systems thereby adsorbing onto and trapping dispersed particles and holding them in a flocculated state.
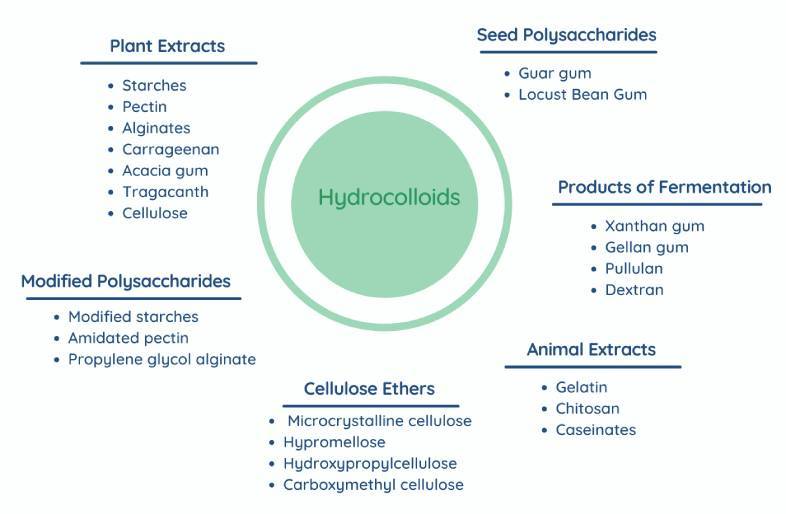
These materials are mainly hydrocolloids although not always, and include:
C). Viscosity modifiers
The deal disperse system is one that displays pseudoplastic or thixotropy behaviour, that is, exhibit high apparent viscosity at low shear rates.
Upon storage, the dispersed particles either settle slowly or, and preferably, remain suspended. When the product is sheared, for instance, when shaken by the consumer, the high apparent viscosity of the formulation should fall sufficiently for product to be dispensed easily.
The various materials currently used as viscosity modifiers are outlined below:
1. Polysaccharides
Examples of polysaccharide-based viscosity modifying excipients include the following:
2. Water-soluble cellulose ethers
Several cellulose ethers have the ability to increase viscosity of aqueous systems in which they are dispersed. They include:
The viscosity-increasing properties of cellulose ethers depends on the molecular weight and degree of substitution.
3. Hydrated silicates
Hydrated silicates are naturally-occurring siliceous clays that exist as colloids in water. This group of pharmaceutical grade clays includes:
- Bentonite
- Hectorite
- Magnesium aluminium silicate (VEEGUM®)
Hydrated silicate materials exhibit thixotropic behaviour at low concentration in water and as gels at high concentration.
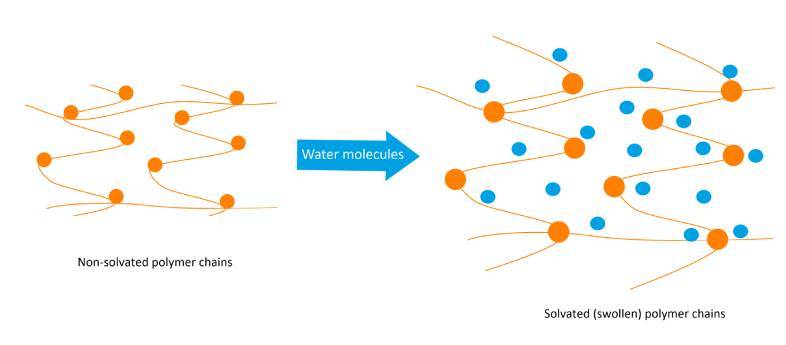
Carbomers are high molecular weight cross-linked polyacrylic acid polymers that swell in water to form viscous hydrogels depending on the degree of cross-linking.
Among carbomer excipients, carbomer 940 is the most commonly used suspending excipient in both topical and oral products.
If you would like to learn more about carbomers, here is a link to an article that gives an overview on these important excipients:
D). Density modifiers
From probing Stokes’ law above, it is clear that if the densities dispersed and dispersing medium are of the same magnitude sedimentation would be significantly slowed down.
Thus, changing the density of the dispersing medium, for example, addition of glycerol, propylene glycol, polyethylene glycol or sucrose-based syrups, can significantly modify densities and leveraged to control instability.
You read more about viscosity modifying excipients through this link:
Summary of Pharmaceutical Suspending Agents
Many pharmaceutical products are formulated as disperse systems in which particulate solids (active ingredients and/or excipients) are distributed throughout a continuous or disperse phase. Owing to the tendency towards settling or creaming by the disperse phase, the use of suspending agents is mandated.
There are many different types of pharmaceutical suspending agents; they can be grouped into four main classes depending on the mechanism of function:
Careful selection of suspending agents is essential in order to have a product that ensures the disperse phase does not settle rapidly, the particle do not settle into a cake, the system is easily re-dispersed into a uniform mixture when shaken, is easy to dispense from the container or use by the consumer.